Saol Therapeutics Pipeline
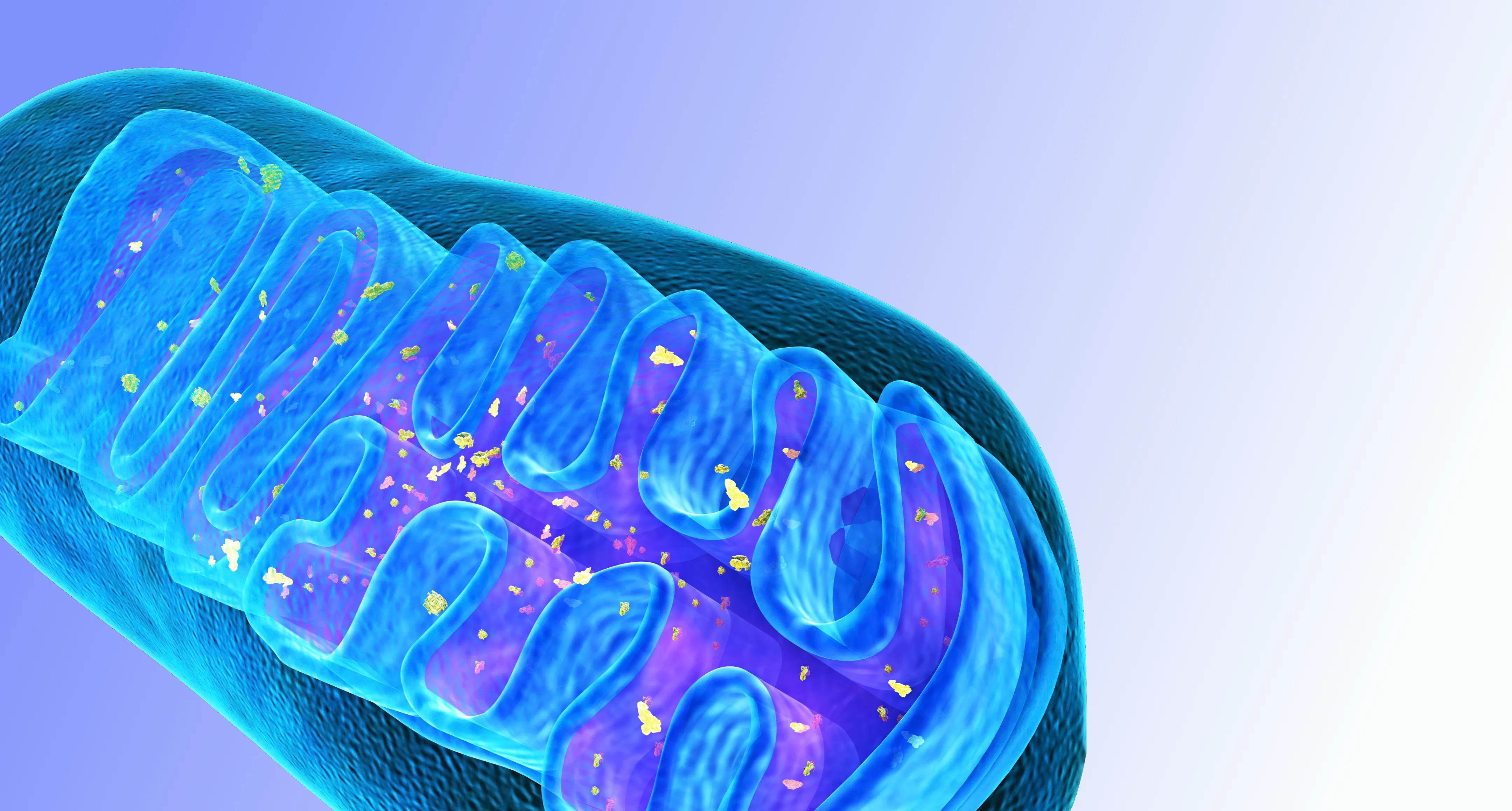
Pyruvate Dehydrogenase Complex Deficiency (PDCD)
Approximately 90 Births per Year 29
Oral Solution
NCT02616484
- Professor of Medicine, Biochemistry and Molecular Biology
- College of Medicine
- University of Florida
Program Highlights
- Phase III Enrollment Complete
- First potential approved treatment for PDCD
- Individualized genetically driven dosing
- Supported by grants from the NIH and FDA
- Rare Pediatric Disease Designation, US Orphan Drug Designation
Phase III Clinical Trial Summary
This Phase III randomized, placebo-controlled, double-blind trial of 34 children, aged 6 months through 17 years, with confirmed diagnosis of PDC Deficiency. A novel Observer reported outcome (ObsRO) validated survey was completed by study participant's parent/caregiver is the primary efficacy outcome measure.
Expanded Access for SL1009
For more information on Saol Therapeutics' Expanded Access Program, please click here.
Disease Background25-27
Pyruvate dehydrogenase complex deficiency (PDCD) is a mitochondrial disorder of carbohydrate oxidation that mostly affects the brain and leads to decreased ATP production and energy deficit. Symptoms of PDC deficiency include signs of metabolic dysfunction such as extreme tiredness (lethargy), poor feeding, and rapid breathing (tachypnea). Other symptoms may include signs of neurological dysfunction such as developmental delay, periods of uncontrolled movements (ataxia), low muscle tone (hypotonia), abnormal eye movements, and seizures. Symptoms usually begin in infancy, but signs can first appear at birth or later in childhood. Symptoms may be especially apparent during times of illness, stress, or after meals with high amounts of carbohydrates. Several hundred children with PDCD have been reported, but the overall frequency is unknown. More males than females are affected by X-linked PDCD. Female carriers of X-linked PDCD may be less severely affected and more difficult to diagnose.
PDCD is caused by abnormalities in the genes that encode the components of the pyruvate dehydrogenase complex. The pyruvate dehydrogenase complex contains three enzymes, E1, E2, and E3, and multiple coenzymes. The E1 enzyme is comprised of an alpha and a beta subunit. PDCD is most commonly caused by abnormalities in the gene that encodes the E1 alpha subunit, E1-alpha subunit pyruvate dehydrogenase gene or PDHA1. The most common form of PDC deficiency is caused by genetic changes (genetic changes or pathogenic variants) in the PDHA1 gene. These pathogenic variants are inherited in an X-linked manner. Pathogenic variants in other genes including PDHB, DLAT, PDHX, DLD, and PDP1 can also cause PDC deficiency. These pathogenic variants are inherited in an autosomal recessive manner.
There are no FDA-approved therapies available for PDCD. Treatment recommendations are based on open label case reports and small trials. Ketogenic diet is the gold-standard therapy for individuals with PDCD because they do not metabolize carbohydrates effectively. Some affected individuals respond to treatment with thiamine, a cofactor for the E1 subunit of the pyruvate dehydrogenase complex.
Pain Related to Osteoarthritis (OA) of the Knee
27M Patients 28
Chemoneurolytic Injection

- Vice Chair and Associate Professor
- Chief of Spine and Musculoskeletal Medicine
- University of Utah
Program Highlights
- Phase II Enrollment Complete
- Proprietary, optimized formulation
- Well-characterized molecule
- Potential blockbuster, multi-indication franchise
Phase II Clinical Trial Summary
This is a multi-center, randomized, double-blind, placebo-controlled single-ascending dose escalation study intended to assess the safety, and efficacy of SL1002 for patients with knee pain associated with osteoarthritis. The study enrolled 4 cohorts for a total of 132 patients. Patients were randomized to receive either SL1002 or placebo in a 3:1 ratio. The study period will be up to 26 weeks, with an additional screening period of up to 2 weeks.
Disease Background
Osteoarthritis of the knee results from an imbalance between breakdown and repair of the tissues in the synovial joint organ and occurs as a result of multiple risk factors including trauma, overuse, and genetic predisposition.1 This condition is characterized by pain, stiffness, and loss of function, which negatively impact on health-related quality of life.2,3 It is one of the leading causes of disability4, with a lifetime risk of painful knee OA approaching 45%5 and expected to rise significantly in the coming decades as the population continues to age.6
Today, symptomatic knee OA is estimated to affect approximately 27 million people in the US alone. It carries a significant economic burden, with estimates of related annual healthcare costs approaching $15 billion dollars.7, 8, 27
Nonsurgical management of knee osteoarthritis includes weight loss, activity modification, and physical therapy. Other treatments include nonsteroidal anti-inflammatory drugs (NSAIDs), oral opioids, and intra-articular corticosteroid injections. However, each of these comes with potential risks and limitations.9,10
If conservative and injection-based therapies fail to provide relief, this condition is frequently treated by total knee arthroplasty (TKA).11 However, many patients – with some estimates as high as 25% of patients suffering from pain related to knee osteoarthritis - are poor candidates for TKA due to a variety of health and non-health related reasons, and they may elect to continue with nonsurgical management.12,13
For patients who do elect to undergo a TKA, chronic post-surgical pain has been reported in 8-34% of patients,14 with an estimated 3.8% eventually requiring revision surgery.15
These statistics, combined with the ongoing opioid crisis, have recently led to a call for the “development of non-opioid-focused multimodal pain management formulations” by global thought leaders16, signaling a significant need for additional non-surgical, therapeutic alternatives.
Spasticity
4M Patients
Chemoneurolytic Injection

- The Wulfe Family Chair of Physical Medicine and Rehabilitation, McGovern Medical School - UTHealth
- Chairman and Professor (with tenure), Distinguished Teaching Professor, UT Systems
- Chief Medical Officer and Clinical Scientist, TIRR Memorial Hermann
- Director, UTHealth NeuroRecovery Research Center at TIRR Memorial Hermann

- Professor, Department of Physical Medicine and Rehabilitation (PM&R) at McGovern Medical School at UTHealth Attending Physician, TIRR Memorial Herman
- Director, Stroke Rehabilitation and Recovery Research, TIRR Memorial Hermann Hospital
- Director, Neurorehabilitation Research Laboratory, UTHealth NeuroRecovery Research Center at TIRR Memorial Hermann
- Professor, Department of Physical Medicine and Rehabilitation - Medical College of Wisconsin
- Director, Stroke Rehabilitation & Spasticity Management – Medical College of Wisconsin and Froedtert Hospital
Program Highlights
- Phase II Enrollment Complete
- Proprietary, optimized formulation
- Well-characterized molecule
- Potential blockbuster, multi-indication franchise
Phase II Clinical Trial Summary
A multi-center, randomized, double-blind, placebo-controlled single ascending dose escalation study intended to assess the safety, pharmacokinetics and efficacy of a single treatment of SL1002 in patients with mild to severe limb spasticity. The study enrolled 4 cohorts of 8 patients per cohort for a total of up to 32 patients. Patients were randomized to receive either SL1002 or placebo in a 3:1 ratio. The study period will be up to 26 weeks, with an additional screening period of up to 2 weeks.
Disease Background
Spasticity is a motor disorder characterized by velocity-dependent increase in tonic stretch reflexes resulting from an upper motor neuron lesion, presenting as intermittent or sustained involuntary activation of muscles. Clinically, this results in increased muscle tone, exaggerated tendon reflexes, clonus and re-emergence of primitive reflexes.17
Disorders of the central nervous system, such as strokes, traumatic brain injuries, cerebral palsy, multiple sclerosis and spinal cord injuries result in neural reorganization causing abnormal neural and muscle control. Spasticity develops because of an imbalance between excitatory and inhibitory input to motor neurons resulting in disinhibition of the stretch reflex and increased muscle excitability. The pattern of spasticity depends on the location of the injury in the CNS. Alterations in neural pathways lead to changes in mechanical properties of muscles and joints that account for some features of spasticity.18
It is estimated that spasticity effects over 12 million people worldwide19 including over 4 million in the United States alone.20 The epidemiology of spasticity is specific to the type and severity of CNS injury. For example, it is estimated that spasticity affects 65-78% of chronic spinal cord injury (SCI) patients21, 25% of stroke patients22, 80% of patients with MS at some point during their clinical course23 and more than 80% in patients with Cerebral Palsy.24